
Messages from STEM and Health Science Scholars
Discourse Analysis: The Impact of the Unspoken Word
Article Excerpt with Reflection
Donna Cempa-Danziger
Abstract
Changes in nursing ethics curriculum and pedagogy are of crucial importance now more than ever. Increasing diversification of patient populations (Wilson-Stronks, Lee, Cordero, Kopp & Galvez, 2008) demands that healthcare providers become trained in ethical and empathetic care of people of various cultures, languages, class, gender, and religion. Cultural norms may cause patients to have views of their sense of disease and treatment that differs from our society. Healthcare providers need training to be aware of and sensitive to such differences. Current ethics training may not provide a solid background for new nurses to be comfortable with decision making in treatment decisions. Additionally, there are discrepancies in teaching ethics as well as where to insert ethics content. Some curricular design suggest to insert such ethics content throughout course training (Numminen, van der Arend, & Leio-Kilpi, 2009). Other research has suggested that effective ethics training should occur occurs through singular courses (Gaul, 1987; Gorgulu & Dinc, 2007). Additionally, there is also concern over the quality of instructor knowledge in conducting ethics training (Borhani, Alhani, Mohammadi & Abbaszadeh, 2010). One approach to comprehensive ethics training is to examine current pedagogy and curriculum design through an intersectionality approach as well as through nursing ethics. Intersectionality examines how race, class, gender, and culture overlap and intersect to define individuals and their experiences. By utilizing both approaches, students will gain a greater understanding and foundation for treating diverse people with dignity and quality care.
Introduction
“We need nursing scholarship that conceptualizes the intersection of class, racialization, gender relations, and other social relations, because we experience our lives not solely as gendered persons, but as classed and racialized persons.” (Anderson, 2006, p. 226)
There is a critical need to address current nursing pedagogical practice. This need includes the training of nurses to meet the needs of an ever-diversifying population. An increasing influx of patients of differing cultures and languages has left gaps in the education of nurses. These gaps include cultural differences, language barriers, knowledge of cross-cultural diseases, and ability to make ethical decisions pertaining to the care of patients and clients (Campesino, 2008). The present nursing program curriculum at **** College, a demographically diverse community college, does not fully address these gaps in a way that will enable nurses to respond to and execute the needs of their patients appropriately. Current courses of study utilize textbooks which are written for White, middle-class populations, leaving nurses ill-equipped to respond to culturally diverse patient needs. This paper proposes a mapping of the current curriculum through the theory of intersectionality. Intersectionality is the examination of how race, class, gender, and culture overlap and intersect to define individuals and their experiences.
Limitations of Intersectionality and Nursing Ethics
While both intersectionality and nursing ethics are valid tools to elicit pedagogical change, there are limitations. Perhaps the greatest challenge is in changing the majority perspective (Lyiscott, 2019; Velazquez, 2016). People may be resistant to change and could be unresponsive to changes in practice and beliefs. It is crucial in this global society to promote awareness of unjust practices, including legal policies as well as educational pedagogy (Kuczewski & Zaidi, 2017). Conversations surrounding intersectionality are uncomfortable within dominant groups not willing to move away from a position of power or unwilling to acknowledge their role in the perpetuation of oppression (Lyiscott, 2019).
The concept of intersectionality is expansive (Muntinga, 2016). It is daunting to begin the task of how so many variables overlap and how to address specialized needs. Meeting healthcare requirements specialized for ethnicity, gender, and culture, compounds needing the use of intersectionality in healthcare. Attempting to educate nursing students in the ethical and culturally responsive care of such a broad population may be impossible. Do we educate towards the majority or try to address every background? Where is the line drawn? In addition, as intersectionality and nursing ethics meet, some cultures may have different ethical positions than the healthcare provider. How do we, as educators, address potential clashes between beliefs of the patient versus the healthcare provider?
Nursing ethics, as it relates to intersectionality, has several foundational limits. Most textbooks are written by White, middle-class men and do not address the health needs of our diversifying society and its needs (Van Herk, 2011). Nurses, in general, have to take a submissive position to medical colleagues regarding ethical and healthcare issues (Wood, 2005, p. 6). Decisions made by nurses may be met with disapproval or dismissed. There is also a need to keep up ethics pedagogy with ever advancing biomedical advances (Wood, 2005). Many younger nurses, while receiving some ethical training, may not possess the confidence to assert ethical decisions (Martin, 2006). A final foundational limit is the role of care as it applies to intersectionality. There is a duality in care ethics as it applies to intersectionality. While nurses may run the risk of harboring subconscious bias towards patients based on their ethnicities, culture, and socioeconomics, patients may also possess such feelings (Campesino, 2008). Discrimination may cause some patients to resist being cared for by nurses due to ethnic and cultural differences.
Discourse Analysis
Discourse analysis is a tool to examine if there is a need to change the current bioethics curriculum. Discourse analysis examines the use of language and how it relates to social context (Rogers, Malancharuvil-Berkes, Mosley, Hui & O’Garro Joseph, 2005). Fairclough established a means of language analysis, which is known as Critical Discourse Analysis (CDA). According to CDA, there are three dimensions to analyze language and its role in society. The first is text, which has multiple interpretations based on the words we choose. Words can reflect underlying attitudes. The second is discursive practice. The words and language used can lead to change, or have the societal dynamic remain the same. Words can present certain values. The last way we can analyze discourse is how words mold societal views and affect social practice (Fairclough, 1992).
This paper examines the use of discourse through intertextual chains (Jorgensen & Philips, 2002). In this process, one examines multiple texts and looks for common themes. For this paper’s purposes, the common themes include a need for reform in where ethics is taught within nursing programs as well as a need in reform as to how to teach ethics. This includes a need for reform in incorporating intersectionality within nursing ethics programs as well as the provision of qualified instructors.
Using Fairclough’s three-dimensional model, we can see the following: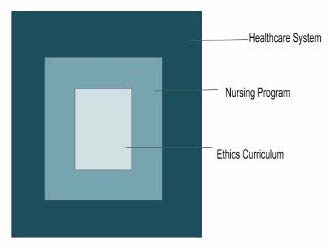 In this analysis, the meta-level explores the current bioethics curriculum within the prenursing program at *** College. The topics taught within the course are analyzed. The mesolevel examines material presentation, including how and where, within the pre-nursing/nursing program. The macro-level includes how the healthcare system incorporates this material. Discourse on the macro-level includes the examination of how the healthcare organization supports or dismisses the role of nurses in executing ethical decisions, as well as how young nurses are suppressed and dismissed by higher-level or more experienced colleagues (Van Herk, 2011). Missing from the conversation is how to teach ethics with an intersectional approach.
In this analysis, the meta-level explores the current bioethics curriculum within the prenursing program at *** College. The topics taught within the course are analyzed. The mesolevel examines material presentation, including how and where, within the pre-nursing/nursing program. The macro-level includes how the healthcare system incorporates this material. Discourse on the macro-level includes the examination of how the healthcare organization supports or dismisses the role of nurses in executing ethical decisions, as well as how young nurses are suppressed and dismissed by higher-level or more experienced colleagues (Van Herk, 2011). Missing from the conversation is how to teach ethics with an intersectional approach.
Need for Curricular Change
Many nursing ethics training programs fall short in providing students with a firm foundation for ethical decision making nor being adept at contributing to the current healthcare environment (Wood, 2005). There is little time allotted to ethics education with many programs offering few, if any, stand-alone nursing ethics courses. The curriculum only allows modules interspersed throughout degree programs. Students and faculty may not realize the importance of ethics training. Many students find the classwork uninteresting and unimportant (Park, Kjervik, Crandell & Oermann, 2012). The lack of qualified instructors is a final concern with ethics training (Ion, 2018). There is a discrepancy in student decision-making confidence based on being taught by an expert versus non-expert instructor (Lin, Lu, Chung and Yang, 2010). All of the above have led to a lack of confidence by nurses in making ethical decisions.
Van Herk (2011) has pointed out a need for discourse regarding “power relations” within nursing interactions. Struggles between colleagues, doctors, and at the institutional level can impede the ability of nurses to provide quality care. Improving nursing ethics education through an intersectional approach can better equip nurses to address oppression, privilege, and promote social justice (p. 30). According to post-colonial feminism, we need a healthcare system that will respond to the differing social positions of patients (Anderson, 2002). Additionally, an intersectional approach to nursing ethics education may “assist with racism and struggles which occur on the colleague as well as care recipient levels” (Ion, 2018, p. 4). Global nursing is a branch of an intersectional approach. The goal of global nursing is to cultural sensitivity, with nurses collaborating globally to relieve suffering and “safeguard human dignity” (Holmgren, 2017). The basis of this perspective is the premise that diseases and empathetic quality care have borders. Holmgren (2017, p.172), emphasized the “need to address global issues to develop knowledge regarding healthcare, people, suffering and ecology in local and global context.”
Reflection
“The most difficult and complicated part of the writing process is the beginning.”
– A. B. Yehoshua
Writing any paper has been a struggle for me due to my being out of school for over 30 years. Most of my recent writing is for doctoral course work. When I began the doctoral program, my writing was less than “academic” or “professional.” With each paper I write, I find that I have improved my higher-order thinking. My current work on a book chapter has also challenged my ability to synthesize ideas and find my voice. A technique I have been using while I work is writing down terms with definitions that I am not familiar with. This has greatly improved my working vocabulary and provided me with a personal synonym list. One great challenge I have faced is staying focused and on task. My normal writing schedule consisted of writing for hours on the weekends. One of my instructors suggested that I instead write every day in 15-minute chunks, then take a break. This timing is based on studies of cognitive focus, which have shown that our ability to stay focused is limited to 15-minute segments. A brief explanation is found within this link: https://jovanevery.co.uk/15-min-writing-challenge/.
The preceding paper was written for a doctoral course on curriculum design and took approximately two months to write, with the finished product being 28 pages. I have included only certain aspects of it, since its purpose was to redesign a course or program. What makes this paper unique is not the premise, but the technique used—discourse analysis. I had never heard of this type of paper or the term other than knowing discourse involved a “conversation.” A discourse paper looks at word use and how it may reflect current societal thinking or create change. My paper focused on what was missing in the conversation regarding teaching nursing ethics, and that is intersectionality. Not every paper has to present words already said or written; sometimes the most powerful ideas come from what isn’t said. The use of discourse analysis enables the writer to look at what is missing from conversations.
Sometimes when we are given a writing task, we are not aware of its future use. At the time that this paper was written, I truly could not see the purpose or use of discourse analysis in my future work. Since beginning my dissertation writing process, I am seeing the relevance of this type of writing analysis. My dissertation topic uses feminist methodology which looks at unspoken words and conversations. Writing this paper has given me a foundation and practice for my data analysis, which is based on interviews of female faculty. I will be analyzing the interview for what is implied and not overtly stated in addition to what is said.
When beginning any paper, I conduct a Google scholar search on the topic. From the initial search, I select a few papers to scan over, looking for in situ citations that may lead me to more references on my topic of interest. Sometimes I will find an article that is so well written and organized that I emulate the style. I begin every paper with a “hook” which can be a quote or statistic. The goal is to capture readers’ attention and make them want to read more. The quote I chose for this paper sets the stage for the paper’s purpose and is much more interesting than saying “The purpose of this paper is….” The paper goes on to provide a more detailed explanation of the purpose, as well as a brief outline of the paper’s direction. By providing an outline, the reader is given an idea of what to expect. When I am scanning papers for review, I will sometimes look for the outline to decide what areas I want to jump to for fast reading. I also tend to include in the introduction brief definitions of terms that the reader may not be familiar with. This particular paper includes a visual representation of Fairclough’s three-dimensional model of discourse analysis as it relates to my area of study. The chart provides the reader with a more tangible understanding of the content within the discourse analysis.
My personal writing technique is to “vomit” my ideas onto paper. This allows me to get all my thoughts out at once. I will then try to arrange my ideas into somewhat organized paragraphs. As I write, I re-read previous sections and edit. I do not track my editing, choosing rather to delete and rewrite. Sometimes I will move a sentence down and rewrite it above to decide which one I prefer. I usually walk away from my writing for ten or fifteen minutes before doing any editing, repeating the process in between fits of writing. Once I have finished the writing and editing process, I edit one last time by reading my work aloud. It’s shocking how different the writing sounds when you hear it aloud instead of reading it. A final step in my writing is sending it to an editor who spends most of the time catching my active–passive errors. I would say that in addition to struggling with academic writing, my active–passive usage is poor.
Realize that writing is a slow process and a true labor of love. I hope that by discussing my experience, I have shown you that all writing is important, that writing in short chunks can be more efficient than spending three hours all at once, and lastly, you must edit, edit, edit.
References
Anderson, J. M. (2006). Discourse/Discours-Exploring Intersections: Does Racialization Matter?. Canadian Journal of Nursing Research Archive, 7-14.
Anderson, J. M. (2000). Gender, ‘race’, poverty, health and discourses of health reform in the context of globalization: A postcolonial feminist perspective in policy research. Nursing inquiry, 7(4), 220-229.
Borhani, F., Alhani, F., Mohammadi, E., & Abbaszadeh, A. (2010). Professional Ethical Competence in nursing: the role of nursing instructors. Journal of Medical Ethics and History of Medicine, 3.
Campesino, M. (2008). Beyond transculturalism: Critiques of cultural education in nursing. Journal of Nursing Education, 47(7), 298-304.
Fairclough, N. (1992). Discourse and Text: Linguistic and Intertextual Analysis within Discourse Analysis. Discourse & Society, 3(2), 193–217. https://doi.org/10.1177/0957926592003002004
Gaul, A. L. (1987). The effect of a course in nursing ethics on the relationship between ethical choice and ethical action in baccalaureate nursing students. Journal of Nursing Education, 26(3), 113-117.
Görgülü, R. S., & Dinç, L. (2007). Ethics in Turkish nursing education programs. Nursing Ethics, 14(6), 741-752.
Holmgren, J. (2017). Global nursing: educating future nurses for tomorrow’s nursing care needs.
Ion, R., DeSouza, R., & Kerin, T. (2018). Teaching ethics: Intersectionality, care failure and moral courage. Nurse education today, 62, 98-100.
Jørgensen, M., & Phillips, L. J. (2002).Discourse analysis as theory and method. London, : SAGE Publications Ltd. http://doi.org/10.4135/9781849208871
Kuczewski, M. G., Mejias-Beck, J., & Blair, A. (2019). Good sanctuary doctoring for undocumented patients. AMA journal of ethics, 21(1), 78-85.
Kuczewski, Mark G., and Danish Zaidi. “The rescinding of DACA: What should healthcare professionals and academics do?(and Why?).” (2017): 1-3.
Lin, C. F., Lu, M. S., Chung, C. C., & Yang, C. M. (2010). A comparison of problem-based learning and conventional teaching in nursing ethics education. Nursing ethics, 17(3), 373-382.
Lyiscott, J. (2019). Black Appetite. White Food.: Issues of Race, Voice, and Justice Within and Beyond the Classroom. Routledge.
Martin, D. E., & Kipling, A. (2006). Factors shaping Aboriginal nursing students’ experiences. Nurse Education Today, 26(8), 688-696.
Muntinga, M. E., Krajenbrink, V. Q. E., Peerdeman, S. M., Croiset, G., & Verdonk, P. (2016). Toward diversity-responsive medical education: taking an intersectionality-based approach to a curriculum evaluation. Advances in Health Sciences Education, 21(3), 541-559.
Numminen, O., van der Arend, A. & Leio-Kilpi, H. (2009). Nurse Educators’ and Nursing Students’ Perspectives On Teaching Codes of Ethics. Nursing Ethics, 16(1), pp. 69-82. doi:10.1177/0969733008097991
Park, M., Kjervik, D., Crandell, J., & Oermann, M. H. (2012). The relationship of ethics education to moral sensitivity and moral reasoning skills of nursing students. Nursing ethics, 19(4), 568-580.
Rogers, R., Malancharuvil-Berkes, E., Mosley, M., Hui, D., & Joseph, G. O. G. (2005). Critical discourse analysis in education: A review of the literature. Review of educational research, 75(3), 365-416.
Valenzuela, A. (Ed.). (2016). Growing critically conscious teachers: A social justice curriculum for educators of Latino/a youth. Teachers College Press.
Van Herk, K. A., Smith, D., & Andrew, C. (2011). Examining our privileges and oppressions: incorporating an intersectionality paradigm into nursing. Nursing inquiry, 18(1), 29-39.
Wilson-Stronks, A., Lee, K. K., Cordero, C. L., Kopp, A. L., & Galvez, E. (2008). One size does not fit all: Meeting the health care needs of diverse populations. Oakbrook Terrace, IL: The Joint Commission.
Woods, M. (2005). Nursing ethics education: are we really delivering the good (s)?. Nursing ethics, 12(1), 5-18.
Yehoshua, A. B. (ND). https://quotefancy.com/quote/1477728/A-B-Yehoshua-The-most-difficult-and-complicated-part-of-the-writing-process-is-the
